What Is Microsatellite Instability (MSI)?
Definition
Microsatellite instability (MSI) happens when errors in DNA replication go unchecked, causing mutations in microsatellites—short, repetitive DNA sequences. Under normal circumstances, the DNA mismatch repair (MMR) system detects and corrects these errors. But when this mechanism fails, instability creeps in, leading to an accumulation of mutations that may trigger cancerous changes.
Mechanism
Microsatellites are scattered throughout the genome like genetic signposts. If the MMR system malfunctions—often due to mutations in genes like MLH1, MSH2, MSH6, or PMS2—these signposts become unreliable. The result? Uncontrolled alterations in microsatellite regions, which can pave the way for tumor formation and cancer progression.
Causes of MSI
What triggers MSI? A variety of genetic and epigenetic factors can set this instability into motion:
- Somatic mutations in MMR genes—most frequently MLH1—disrupt repair functions.
- Inherited mutations, like those seen in Lynch syndrome, increase hereditary cancer risk.
- Epigenetic silencing, particularly MLH1 promoter hypermethylation, turns off crucial repair genes.
Key Features of MSI
- Microsatellites consist of short, repeating DNA sequences (1-6 base pairs) found across the genome.
- Healthy cells rely on the MMR system to ensure microsatellite sequences remain stable during cell division.
- In MSI-affected cells, this regulation collapses, leading to unpredictable changes in microsatellite lengths.
Prevalence and Clinical Impact
MSI is not a rare phenomenon—it plays a key role in cancer biology:
15-20% of colorectal cancers exhibit MSI.
30% of endometrial cancers show MSI, highlighting its diagnostic importance.
15% of gastric cancers also harbor MSI, influencing treatment approaches.
More than just a genetic anomaly, MSI acts as a biomarker that helps doctors assess cancer risks, refine diagnoses, and determine personalized treatment strategies, especially in the era of immunotherapy.
Types of Microsatellite Instability
| MSI Classification |
Instability Level |
Description |
| MSI-High (MSI-H) |
High |
High levels of instability; linked to severe genetic alterations. |
| MSI-Low (MSI-L) |
Intermediate |
Moderate level of instability. |
| MSS (Microsatellite Stable) |
None |
No instability detected; normal DNA replication. |
MSI-High (MSI-H)
MSI-High, or MSI-H, refers to a state where microsatellite instability is significantly elevated—usually marked by instability in at least 30% of the genetic markers being analyzed. This level of instability is often associated with severe genetic changes and is commonly found in various cancer types. For instance, in a comprehensive study that explored 39 cancer types, MSI-H prevalence varied, with endometrial carcinoma leading at 31.4%. But what's more interesting? MSI-H tumors often respond more favorably to immune checkpoint inhibitors, making MSI testing a crucial tool for personalizing cancer treatment plans. Research consistently supports the idea that the MSI-H status can predict responses to immunotherapy across multiple cancer types.
MSI-Low (MSI-L)
On the other hand, MSI-Low (or MSI-L) represents an intermediate level of instability. Here, the instability is found in about 15%-29% of the markers being analyzed. While this is not as drastic as MSI-H, it still affects genetic stability and plays a role in cancer development. Interestingly, studies examining different MSI detection methods suggest that MSI-L tumors often present a challenge when it comes to classification, because they fall into a gray area—neither fully fitting the criteria for MSI-H nor MSS (Microsatellite Stable). It's like a middle ground, where things are a bit less clear.
Microsatellite Stable (MSS)
Now, let's look at MSS, or Microsatellite Stable. These are the cancers that show no significant instability—less than 15% of markers exhibit any signs of MSI. In these cases, DNA replication is largely intact, and the microsatellite regions remain stable. But here's where it gets important: MSS tumors are often non-responsive to immune checkpoint inhibitors, which is why MSI testing becomes essential in crafting effective treatment plans. It provides the insights needed to determine whether a patient might benefit from newer immunotherapy treatments, or whether other approaches are needed.
MSI Testing and Analysis: Methods and Technologies
Microsatellite instability (MSI) testing is pivotal in identifying mismatch repair deficiencies in various cancers, notably colorectal cancer. Several laboratory techniques are employed to detect MSI, each with distinct advantages and limitations.
Techniques for MSI Testing
Polymerase Chain Reaction (PCR):
PCR is a widely utilized method for detecting MSI by amplifying specific microsatellite regions and examining them for instability. This technique involves comparing the length of microsatellite sequences in tumor DNA to normal tissue DNA. For example, a study by Peltomäki (2003) showed that PCR is particularly adept at identifying MSI in colorectal cancer, especially in cases linked to Lynch syndrome. And, the pentaplex PCR system, an enhanced version of PCR, takes this even further by offering greater sensitivity and specificity in detecting MSI (Jiang et al., 2018).
If you're looking for a more in-depth approach, NGS is where it's at. It offers a comprehensive look at broader genetic mutations, making it possible to detect MSI with high accuracy. In fact, research has shown that NGS has a 97% concordance with traditional PCR and immunohistochemistry techniques (Pabalan et al., 2020). What makes NGS even more exciting is its ability to analyze multiple microsatellite loci at once, providing deeper insights into the genetic instability of cancer cells. Beyond just MSI, NGS also reveals a wider range of mutations—something that's increasingly crucial in the era of precision oncology.
Immunohistochemistry (IHC):
IHC is another key player in the MSI testing field. It focuses on identifying the loss of MMR proteins in tumor tissues, which is a hallmark of MSI. With the help of antibodies, IHC detects proteins like MLH1, MSH2, MSH6, and PMS2, which are often lost in tumors with MSI. In colorectal cancer, IHC and PCR are typically seen as equivalent when it comes to MSI testing (Ruffin et al., 2019). However, while IHC is great at spotting protein loss, it doesn't always catch every type of MSI—particularly when mutations don't affect protein expression but still disrupt microsatellite stability.
High-resolution melting analysis (HRM):
A more recent method, HRM, is gaining traction as a fast, cost-effective way to detect MSI. HRM measures the melting temperature of DNA fragments to assess sequence instability, and studies like Capelle et al. (2014) have demonstrated that HRM can be a reliable alternative to PCR for detecting small-scale microsatellite changes. Although HRM isn't as widely used as PCR, it has distinct advantages in settings where time and cost are critical factors—like clinical trials or initial diagnostic steps.
Liquid biopsies:
Liquid biopsies are the new frontier in MSI testing. These non-invasive tests, which analyze circulating tumor DNA (ctDNA) found in blood samples, offer the promise of earlier detection and monitoring of MSI-high cancers. A study by Wang et al. (2018) highlighted liquid biopsies as a viable method for detecting MSI across a range of cancers, including colorectal. It's a real game-changer for patients who aren't suitable candidates for traditional tissue biopsies, making it possible to track MSI status over time without the need for invasive procedures.
For more information on MSI testing, see Microsatellite Genotyping Service.
MSI Testing Kits
For clinical use, MSI testing kits like the MSI-IVD kit provide a standardized way to detect MSI. These kits typically use PCR methods to assess tumor-agnostic MSI status, which has been validated for solid tumors—especially those exhibiting MSI-H. Shia et al. (2017) pointed out that these kits offer clinicians an essential tool in personalizing treatment, particularly when considering therapies like immune checkpoint inhibitors for MSI-H cancers.
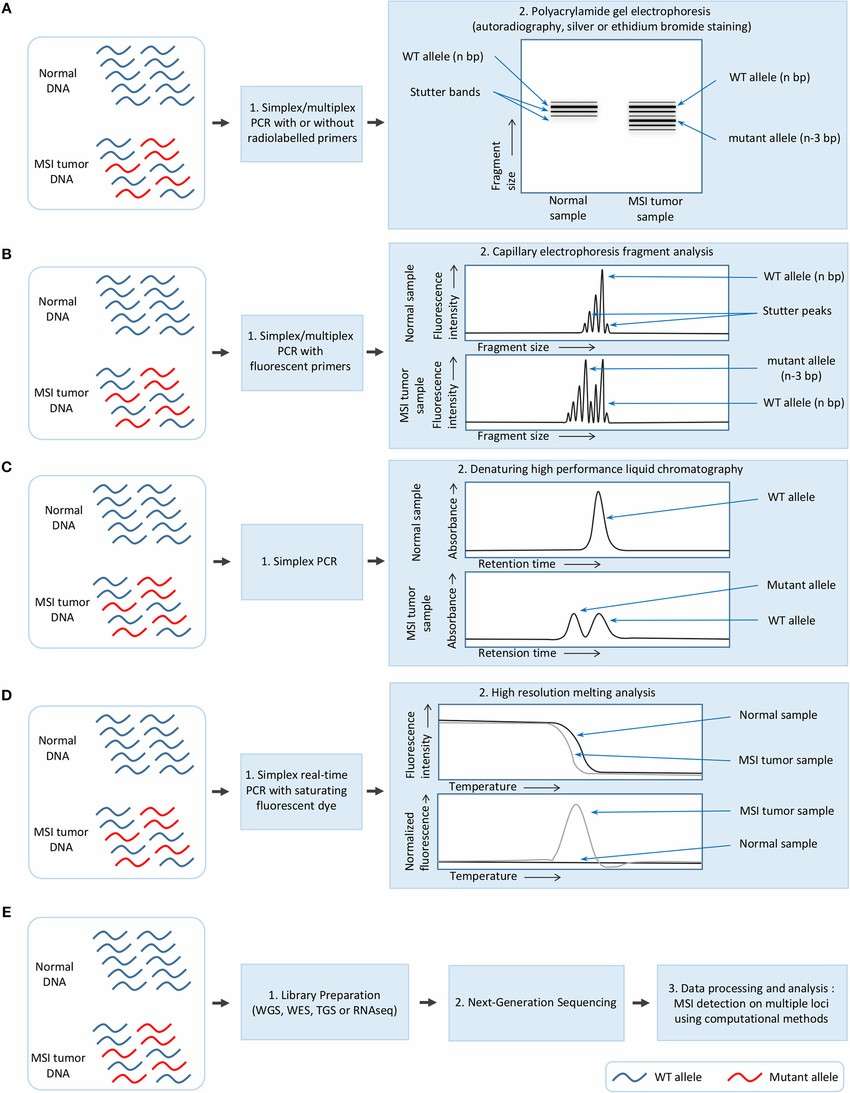 Overview of the different methods used for MSI detection in cancer. (Laura G. Baudrin et al,. 2018)
Overview of the different methods used for MSI detection in cancer. (Laura G. Baudrin et al,. 2018)
Comparison of MSI Testing and Analysis Methods
| Testing Method |
Description |
Advantages |
Limitations |
Applications |
Accuracy & Sensitivity |
| Polymerase Chain Reaction (PCR) |
Amplifies specific microsatellite regions to detect instability by comparing tumor DNA with normal tissue DNA. |
- Widely used and cost-effective
- Highly effective in diagnosing Lynch syndrome
- Established track record in colorectal cancer |
- Less sensitive for detecting small-scale changes
- May miss mutations that do not significantly alter microsatellite length |
- Primary method for MSI detection in colorectal cancer
- Diagnosis of Lynch syndrome and other MMR deficiencies |
- Accuracy: High for detecting MSI in specific loci like in Lynch syndrome.
- Sensitivity: Moderate, especially for larger-scale changes but lower for subtle mutations. |
| Next-Generation Sequencing (NGS) |
Analyzes broad genetic mutations, providing high accuracy for MSI detection by examining multiple loci simultaneously. |
- High accuracy and sensitivity (97% concordance with PCR)
- Analyzes multiple microsatellite loci at once
- Detects a wider range of mutations |
- High cost
- Requires more specialized equipment and expertise
- May not be as widely accessible |
- Precision oncology
- Comprehensive MSI detection across multiple cancer types
- Detailed mutation analysis |
- Accuracy: Very high, as it provides a broad analysis of genetic mutations.
- Sensitivity: Very high, capable of detecting a wide range of mutations and microsatellite instabilities. |
| Immunohistochemistry (IHC) |
Detects the loss of MMR proteins (MLH1, MSH2, MSH6, PMS2) in tumor tissues, a hallmark of MSI. |
- Directly assesses protein loss
- Useful for understanding the presence of MMR deficiencies
- Less invasive than sequencing |
- Cannot detect all forms of MSI
- Does not identify mutations that do not affect protein expression |
- Detecting MSI in colorectal cancer and other cancers with MMR deficiencies
- Used alongside PCR for confirmation |
- Accuracy: Moderate; useful for detecting MSI due to MMR protein loss, but misses certain mutations that don't affect proteins.
- Sensitivity: Moderate to low, as it depends on visible protein loss. |
| High-Resolution Melting Analysis (HRM) |
Measures the melting temperature of DNA to assess sequence instability. Used to detect small-scale microsatellite changes. |
- Cost-effective
- Quick and reliable alternative to PCR
- Suitable for clinical trials and diagnostic settings |
- Less established than PCR
- Not as widely used in routine clinical practice
- Limited by small-scale changes only |
- Small-scale MSI detection
- Clinical trial settings
- Initial diagnostics in resource-constrained environments |
- Accuracy: High for detecting small-scale changes in microsatellite sequences.
- Sensitivity: Moderate; better suited for smaller mutations but may not catch larger, more complex alterations. |
| Liquid Biopsies |
Non-invasive blood tests that detect circulating tumor DNA (ctDNA) to monitor MSI-high cancers. |
- Non-invasive and patient-friendly
- Can detect MSI in various cancer types
- Potential for early detection and monitoring |
- Limited sensitivity in early-stage cancers
- Currently more experimental than established methods |
- Monitoring MSI in real time
- Early detection of MSI-high cancers
- For patients not suitable for traditional biopsies |
- Accuracy: Moderate to high for detecting MSI in advanced stages; more research is needed for earlier stages.
- Sensitivity: Moderate; liquid biopsies are still experimental but show promise for detecting MSI in advanced cancers. |
Microsatellite Instability vs. Chromosomal Instability
| Category |
Microsatellite Instability (MSI) |
Chromosomal Instability (CIN) |
| Cause |
Defects in the DNA mismatch repair (MMR) system |
Defects in chromosomal segregation, telomere stability, and DNA damage response |
| Characteristics |
Alterations in the length of microsatellite sequences |
Widespread imbalances in chromosome number (aneuploidy) and loss of heterozygosity (LOH) |
| Results |
Hypermutable phenotype with multiple point mutations |
Gross chromosomal alterations and abnormal karyotype |
| Cancer Pathogenesis |
- Accounts for ~15% of sporadic colorectal cancers |
- Represents ~85% of sporadic colorectal cancers |
|
- Rapid accumulation of mutations in key regulatory genes |
- Widespread chromosomal alterations and aneuploidy |
|
- Associated with a better prognosis in colorectal cancer |
- Often associated with mutations in tumor suppressor genes and oncogenes |
| Relationship |
Some MSI-H tumors also display varying degrees of CIN |
- |
| Clinical Relevance |
Diagnostic and Prognostic Value: MSI testing identifies Lynch syndrome and guides treatment decisions |
Diagnostic and Prognostic Value: CIN status is linked to more aggressive tumors |
|
Treatment Strategies: MSI-H tumors show better response to immune checkpoint inhibitors |
Treatment Strategies: CIN tumors may respond better to chemotherapies targeting chromosomal instability |
|
Precision Medicine: MSI status aids in personalized treatment approaches |
Precision Medicine: CIN status helps in tailoring treatment for chromosomal instability |
| Conclusion |
MSI and CIN are complex and intertwined pathways of genomic instability that impact cancer development and progression. Their understanding is crucial for better diagnostics and treatment planning. |
Both MSI and CIN play pivotal roles in cancer and require integrated analysis for a more comprehensive understanding of tumor behavior and treatment strategies. |
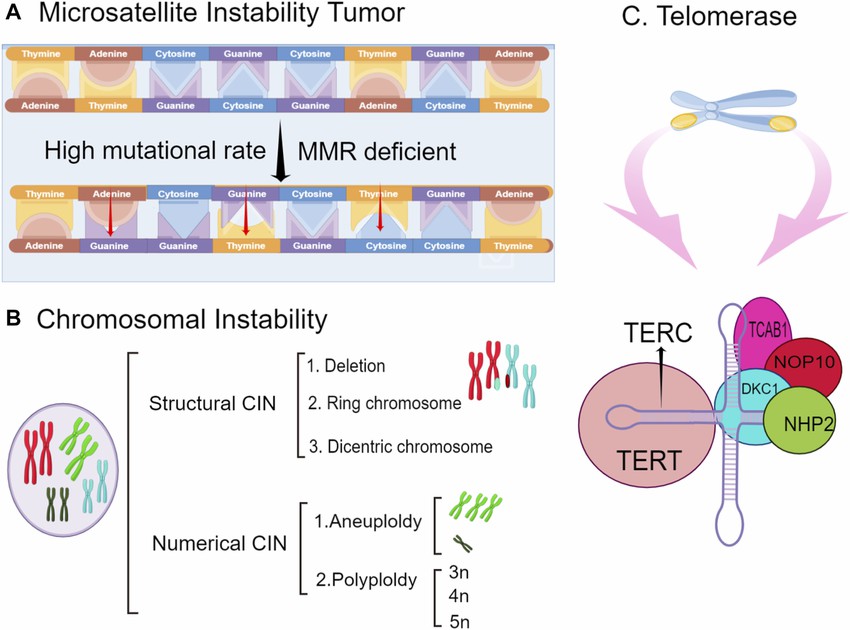 The types of genomic instability include microsatellite instability (MSI), chromosomal instability, and telomerase inactivation. (Menghui Wang et al,.2022
The types of genomic instability include microsatellite instability (MSI), chromosomal instability, and telomerase inactivation. (Menghui Wang et al,.2022
Emerging Research and Advances in MSI
| Aspect |
Key Advances |
| Genetic Insights |
- Ongoing research into Lynch syndrome and hereditary cancer syndromes
- Exploration of MSI's role in other cancer types
- Potential for early detection strategies |
| Diagnostic Advancements |
- Next-generation sequencing (NGS) for MSI detection
- Comprehensive genomic profiling (CGP) for simultaneous MSI and genomic alteration analysis
- Liquid biopsy-based CGP assays for less invasive testing
- AI-based prediction of MSI/dMMR status from histomorphological features |
| Therapeutic Strategies |
Immunotherapy:
- Efficacy of immune checkpoint inhibitors (ICIs) in MSI-high tumors
- Pembrolizumab approval for advanced MSI-H/dMMR tumors
- Need for research on response predictors and immune escape mechanisms
Targeted Therapies:
- Identification of fusion kinases in MSI-H colorectal cancers
- Potential for therapeutic kinase inhibitors
- Link between NTRK fusion and colorectal serrated neoplasia pathway |
| Molecular Insights |
- Mutator phenotype in MSI-driven carcinogenesis
- Hyper-mutated state with increased neoantigen expression
- Favorable, immune-rich tumor microenvironment
- Importance of DNA sensing in cancer cells for antitumor immunity |
| Clinical Impact |
- Newcastle MSI-Plus Assay: high sensitivity and specificity
- Improved Lynch syndrome screening
- Reduced turnaround times
- Increased testing rates and identification of CRC patients at risk of Lynch syndrome |
The Link Between Microsatellite Instability and Cancer
MSI in Colorectal Cancer (CRC)
Colorectal cancer (CRC) is one of the most prominent cancers linked to MSI. Studies show that about 15% of CRCs exhibit MSI, with MSI-High tumors often associated with Lynch syndrome, a hereditary condition that increases the risk of various cancers. MSI testing in CRC is critical for identifying patients who may benefit from targeted therapies, especially immune checkpoint inhibitors.
For more on how MSI testing can aid in CRC diagnosis, visit Microsatellite Instability Analysis.
MSI in Other Cancers
MSI is also found in other cancers, including endometrial cancer, gastric cancer, and ovarian cancer. In endometrial cancer, approximately 25% of tumors show MSI-H, and these tumors often have a better prognosis than those without MSI-H. MSI-H tumors in gastric cancer also show a favorable response to immunotherapy, particularly PD-1 inhibitors.
Clinical Importance
MSI status significantly influences cancer treatment options. For instance, tumors with high MSI (MSI-H) are more likely to respond to immunotherapy drugs like pembrolizumab and nivolumab, which are PD-1 inhibitors. Understanding MSI status is therefore crucial for selecting the right treatment and improving patient outcomes.
Immunotherapy Selection
MSI has emerged as a powerful biomarker for predicting the efficacy of immune checkpoint inhibitors (ICIs) like pembrolizumab and nivolumab. MSI-High tumors are more likely to respond to ICIs, offering new hope for patients with advanced cancers that are resistant to conventional therapies.
Prognostic Value
Studies have shown that MSI-High tumors are often associated with better prognosis, particularly in cancers like colorectal and endometrial cancer. MSI status can help clinicians predict the likelihood of treatment success and adjust strategies accordingly.
The Future of MSI in Cancer Diagnosis and Treatment
Microsatellite instability is a powerful tool in the diagnosis and treatment of cancer. As research continues to advance, MSI testing could become a standard part of cancer screenings, leading to more personalized and effective treatments. New genetic therapies and better understanding of MSI could revolutionize cancer care, offering patients a greater chance of survival and a higher quality of life.
Data and Impact of MSI in Cancer Treatment
Here's a quick glance at the prevalence, prognostic impact, and immunotherapy response rates associated with MSI in various cancers:
| Cancer Type |
MSI Prevalence |
Prognostic Impact |
Immunotherapy Response Rate |
| Colorectal Cancer |
15% |
Associated with Lynch syndrome, better prognosis for MSI-H tumors |
~40-50% with PD-1 inhibitors |
| Endometrial Cancer |
25% |
MSI-H tumors often have better prognosis |
Response rates vary, generally high |
| Gastric Cancer |
20% |
MSI-H correlated with favorable prognosis |
Often responsive to immunotherapy |
| Ovarian Cancer |
~10-15% |
MSI-H linked to improved survival |
Response to checkpoint inhibitors varies |
For more detailed information on MSI testing and related services, visit CD Genomics Microsatellite Instability Analysis.
Conclusion
Microsatellite instability is a game-changer in the fight against cancer. Understanding MSI status provides critical insights into prognosis and treatment response, particularly in personalized medicine. By incorporating MSI testing into clinical practice, we can enhance the effectiveness of cancer therapies, especially immunotherapy. At CD Genomics, we offer advanced services in MSI analysis and testing to help healthcare providers deliver precise and effective cancer treatments.
To learn more about how MSI testing can assist in personalized cancer treatment, visit our Microsatellite Genotyping Service.
References:
-
Jenkins, M. A., Hayashi, S., O'Shea, A. M., Burgart, L. J., Smyrk, T. C., Shimizu, D., ... & Thibodeau, S. N. (2017). Assessment of a streamlined approach to detect Lynch syndrome in colorectal cancer patients. Journal of Clinical Oncology, 35(10), 1082-1089.
- Salipante, S. J., Scroggins, S. M., Hampel, H. L., Turner, E. H., & Pritchard, C. C. (2014). Microsatellite instability detection by next-generation sequencing. Clinical Chemistry, 60(9), 1192-1199.
- Lindor, N. M., Burgart, L. J., Leontovich, O., Goldberg, R. M., Cunningham, J. M., Sargent, D. J., ... & Thibodeau, S. N. (2002). Immunohistochemistry versus microsatellite instability testing in phenotyping colorectal tumors. Journal of Clinical Oncology, 20(4), 1043-1048.
- Hempelmann, J. A., Lockwood, C. M., Konnick, E. Q., Salipante, S. J., & Pritchard, C. C. (2018). MSIsensor: A novel algorithm for characterizing microsatellite instability in cancer genomes. The Journal of Molecular Diagnostics, 20(1), 105-111.
- Bartley, A. N., Luthra, R., Saraiya, D. S., & Urbauer, D. L. (2012). Identification of cancer patients with Lynch syndrome: Clinical performance of the revised Bethesda guidelines and comparison of immunohistochemistry to microsatellite instability testing. The Journal of Molecular Diagnostics, 14(4), 305-311. https://doi.org/10.1016/j.jmoldx.2012.02.003
- Aska, K., et al. (2023). Editorial: Microsatellite and microsatellite instability. Frontiers in Genetics, 14, 1189212.
- Boland, C. R., & Goel, A. (2010). Microsatellite instability in colorectal cancer. Gastroenterology, 138(6), 2073-2087.e3.
- Bonneville, R., et al. (2017). Landscape of Microsatellite Instability Across 39 Cancer Types. JCO Precision Oncology, 1, 1-15.
- De Craene, B., et al. (2021). Comparison of microsatellite instability detection by immunohistochemistry, PCR, and NGS in colorectal and endometrial cancer. Scientific Reports, 11, 12880.

 Sample Submission Guidelines
Sample Submission Guidelines


