
We use cookies to understand how you use our site and to improve the overall user experience. This includes personalizing content and advertising. Read our Privacy Policy
Accept Cookies
Guillain-Barré syndrome (GBS) is a rare, potentially fatal disorder that affects the peripheral nervous system, outside the brain and spinal cord. It is often triggered by a preceding infection and is typically characterized by muscle weakness, loss of tendon reflexes, and in some cases, respiratory difficulties, as well as dysfunctions in autonomic processes such as heart rate and blood pressure regulation. The most prevalent subtype of GBS in Europe and North America is acute inflammatory demyelinating polyneuropathy (AIDP), which primarily targets the myelin sheath and Schwann cells. In contrast, acute motor axonal neuropathy (AMAN) affects the axonal membranes at the nodes of Ranvier. While GBS is classified as an autoimmune disorder, the precise mechanisms that drive its various clinical manifestations are still not fully understood.
A recent study published in Nature investigates the role of the immune system in the development of GBS. The research identified two distinct types of immune cells present in GBS patients. The first type, a subset of CD4+ T cells, has the ability to target a specific antigen in the nervous system. The second type, which is a rare population of CD8+ T cells, also plays a role in the immune response. Among the CD4+ T cells, a particular subgroup, known as TH1 cells, is responsible for initiating the attack. The study further characterized these T cells by their unique features, including polyclonal T cell receptor (TCR) libraries, shorter CDR3β lengths, sensitivity to HLA-DR restriction, and recognition of immunodominant epitopes. These findings were made possible through single-cell RNA sequencing and TCR sequencing. Additionally, the study revealed that the autoreactive TCRβ clonotypes were present in both the blood and cerebrospinal fluid of various GBS patients, but were absent in healthy control subjects. In a final key observation, myelin-reactive T cells were detected in a nerve sample from one patient, indicating their direct involvement in the disease process. These results offer valuable new insights into the immune mechanisms underlying GBS and could have significant implications for future medical applications.
The results of this study suggest that certain viral infections can cause certain immune cells (cytotoxic PNS myelin-reactive CD4+ T cells) to enter the nerves outside the brain and spine. This can lead to local swelling and the arrival of other immune cells, which can cause problems with the myelin (the protective layer around our nerves), make the symptoms of the disease worse, and make the immune response stronger.
Presence of specific autoreactive T cells in patients with GBS
The authors used a range of molecular biology techniques to study patients with AIDP (n=15, including non-covid-19 and post-covid-19 GBS, with disease stages including acute and recovery), patients with AMAN (n=4), and patients with hereditary demyelination. These techniques included in vitro screening, single-cell RNA sequencing (scRNA-seq), single T-cell clonogenic generation, and TCR sequencing. The study also looked at patients with Charcot-Marie-Tooth disease (CMT, peroneal muscular dystrophy) type 1 (CMT 1; n=5) patients and T-cell immunity in healthy donors (some of whom had a history of SARS-CoV-2 infection, non-COVID-19 HD, n=15; post-COVID-19 HD, n=6) were studied.
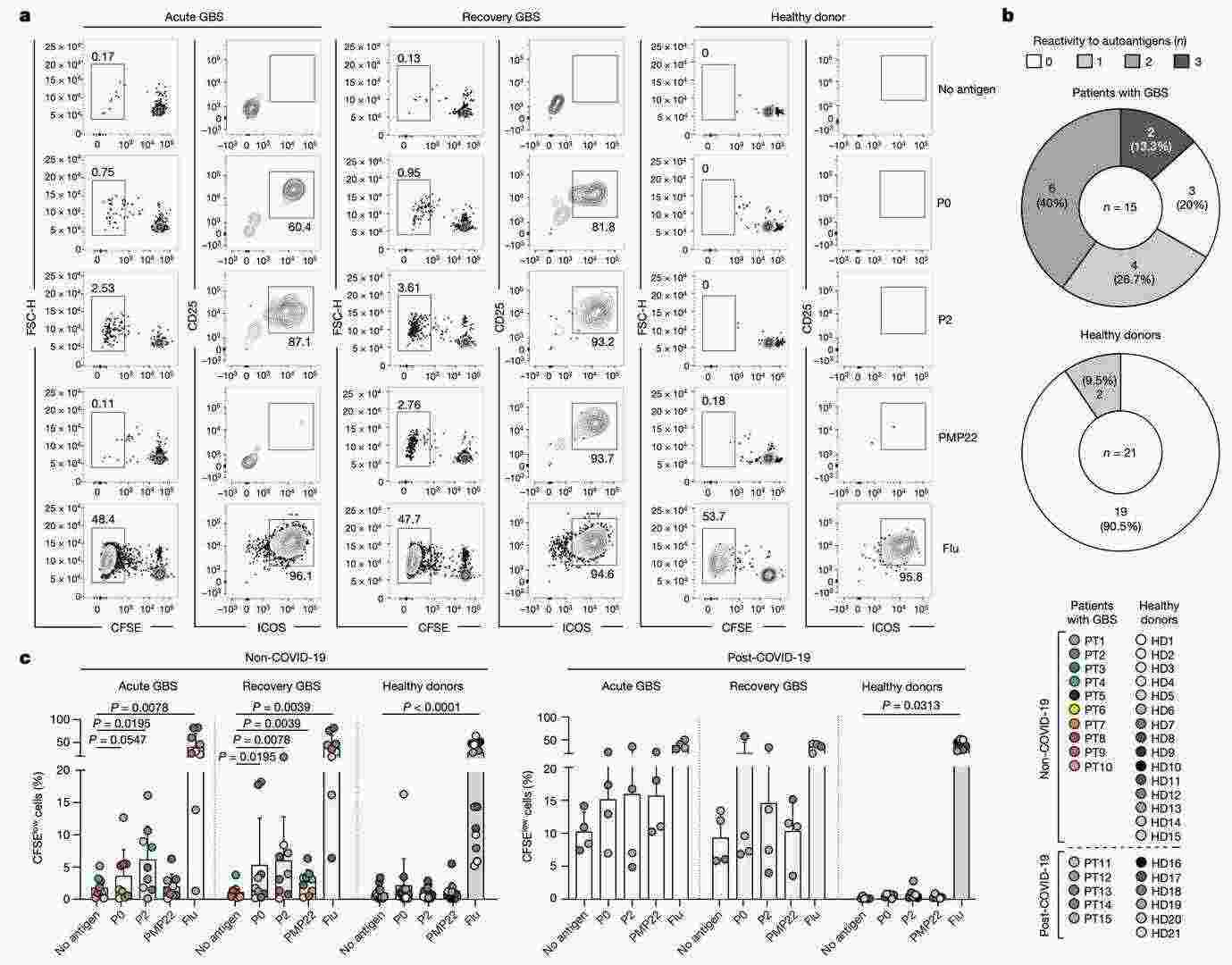 Ex vivo stimulation of memory CD4+ T cells from the blood of patients with GBS and healthy donors (Súkeníková et al., 2024)
Ex vivo stimulation of memory CD4+ T cells from the blood of patients with GBS and healthy donors (Súkeníková et al., 2024)
Using special techniques called 'fluorescence-activated cell sorting' (FACS) and 'co-culture experiments', we found that myelin-reactive memory CD4+ T cells and rare memory CD8+ T cells were present in the blood of most AIDP patients. However, these cells were found to be uncommon in AMAN patients, CMT1 patients and healthy donors. Of these, autoreactive memory CD4+ T cells targeted one or more myelin antigens in the nervous system (i.e. P0, P2 and PMP22) in 12 of the AIDP patients, but largely did not appear to be targeted in the healthy donors (with the exception of 2 of 21).
In addition to this, in non-covid-19 GBS patients, P2 and P0 were the main autoantigens in the acute phase, whereas in the recovery phase there was a significant increase in autoreactive CD4+ T-cell responses to all three PNS myelin antigens. It is interesting that CD4+ T cells from GBS patients after a history of SARS-CoV-2 infection showed increased background proliferation in negative control cultures (no antigen). This supports the idea that GBS may be triggered by infection.
Take the Next Step: Explore Related Services
Autoreactive T-cell clones exhibit high expression of relevant genes
To learn more about the characteristics and TCR pool of autoreactive CD4+ T cells in patients with AIDP, the authors combined in vitro stimulation, single-cell RNA sequencing and paired TCRα and TCRβ (TCRα/β) analysis. The authors extracted memory CD4+ T cells from two patients (PT2 and PT16) and stimulated them in the lab with a myelin antigen (PNS-myelin) or an influenza antigen (flu).
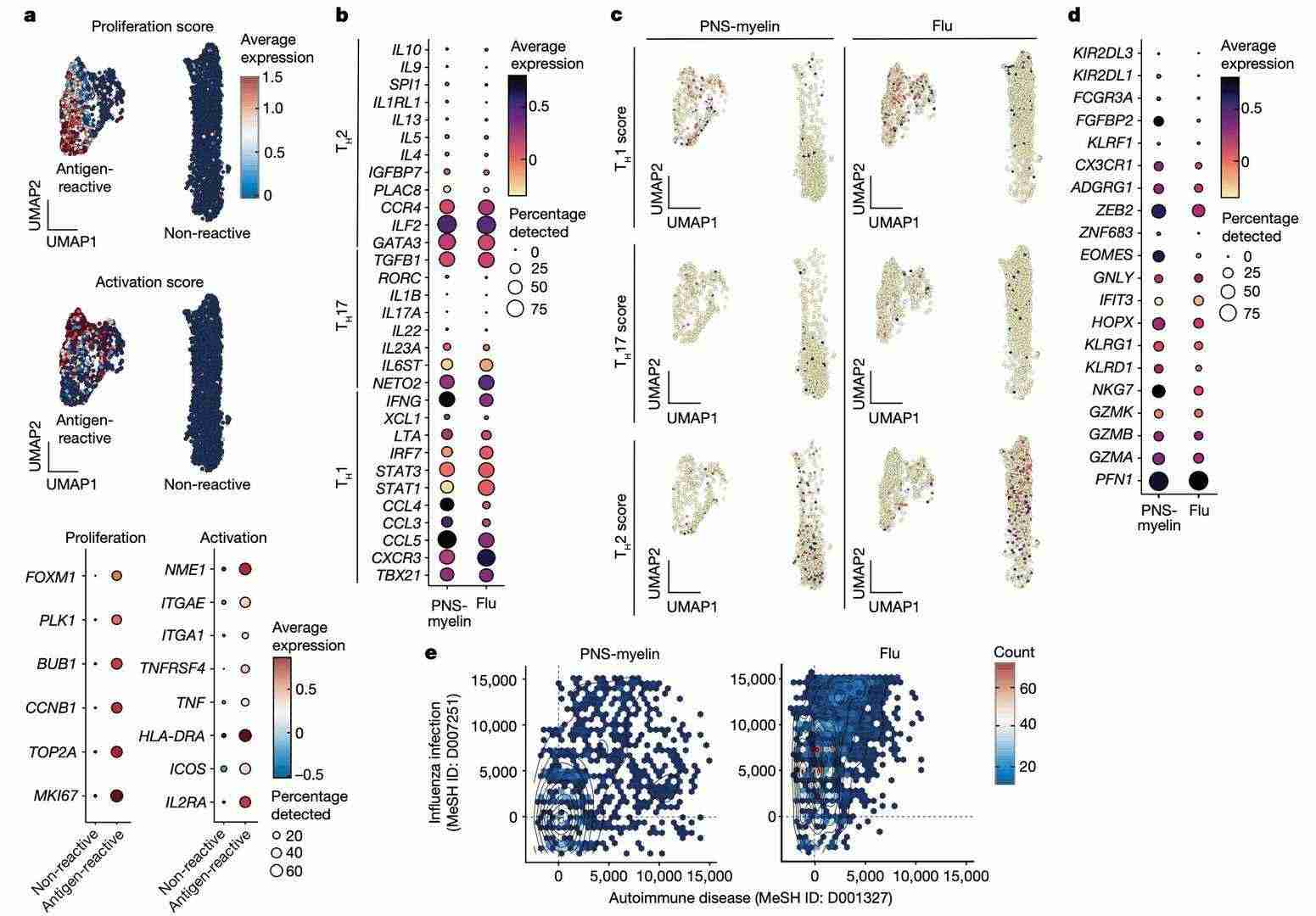 scRNA-seq analysis of memory CD4+ T cells from patients with GBS (Súkeníková et al., 2024)
scRNA-seq analysis of memory CD4+ T cells from patients with GBS (Súkeníková et al., 2024)
When we looked at the data from the study without someone else's help, we could see that there were two different groups. The first group had lots of cells that were growing and becoming active (these cells were called antigen-responsive cells). The second group had cells that didn't respond to a particular antigen, and these cells had low levels of genes that are linked to growth and activity.
Two groups of antigen-reactive T cells are particularly interesting. These are the PNS myeloid and influenza-reactive T cell clusters. Both of these showed high expression of TH1 signature genes, whilst TH2 or TH17 signature genes showed low expression.TH1-related genes were found to be enriched exclusively in antigen-reactive cell clusters. TH2-like signatures were predominantly present in non-reactive cells.
It was interesting to see that, compared to cells that reacted to influenza, cells in the nervous system (PNS) that reacted to myelin showed much higher levels of genes linked to toxicity. In addition, a special type of analysis showed that there were more genes linked to autoimmune conditions in these cells than in cells that reacted to influenza.
Characterisation of autoreactive T-cell clones
To do more research into how the body's own T-cells (a type of cell in the immune system) react in GBS patients, the researchers obtained a total of 987 CD4+ T-cell clones from 13 patients. These were targeting P0 (n=312), P2 (n=520) or PMP22 (n=155). They then looked at the TCRβ clonotypic composition of these T-cell clones, identifying 54 P0-reactive, 88 P2-reactive and 27 PMP22-reactive unique clonotypes.In addition, P0- and P2-reactive T-cell clones with the same TCRβ clonotypes were isolated from blood samples taken during the acute and recovery phase from four GBS patients.
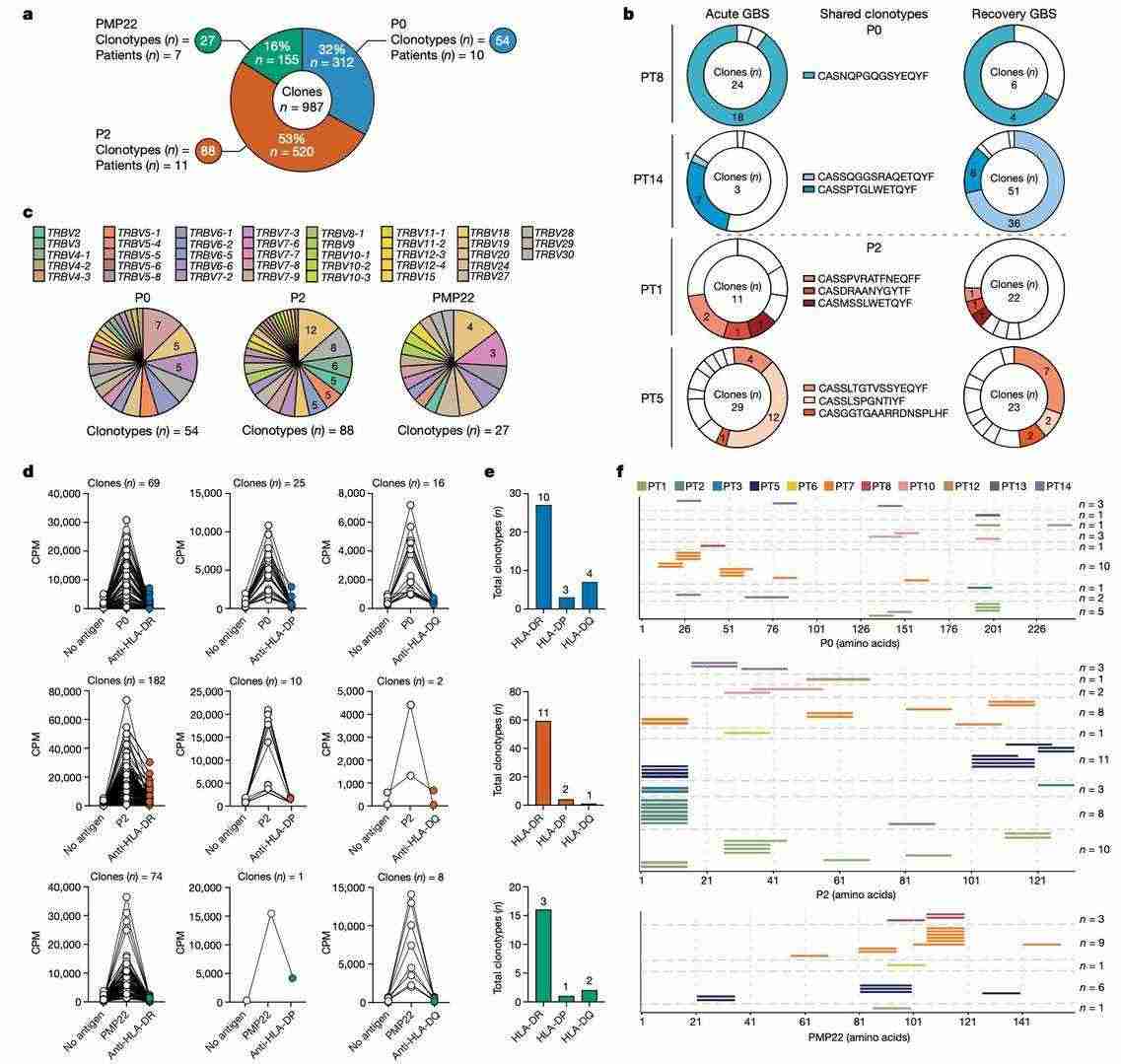 Characterization of autoreactive CD4+ T cell clones from patients with GBS (Súkeníková et al., 2024)
Characterization of autoreactive CD4+ T cell clones from patients with GBS (Súkeníková et al., 2024)
Research showed that a certain type of immune cell (a CD4+ T cell) had a lot of different TCRs. The authors then looked at how human leukocyte antigen (HLA) class II neutralising antibodies (HLA-DR, HLA-DP or HLA-DQ) affected the growth of these CD4+ T cell clones. They found that the cells were mostly affected by HLA-DR. The authors also found that the cells were mostly restricted by HLA-DR. In addition, the authors found that the CDR3β length of PNS myelin-reactive CD4+ T cell clonotypes was shorter than the CDR3β lengths of viral- and bacterial-specific or total memory CD4+ T cells. This supports their autoreactive profile.
TCRβ clonotypes in patients with GBS
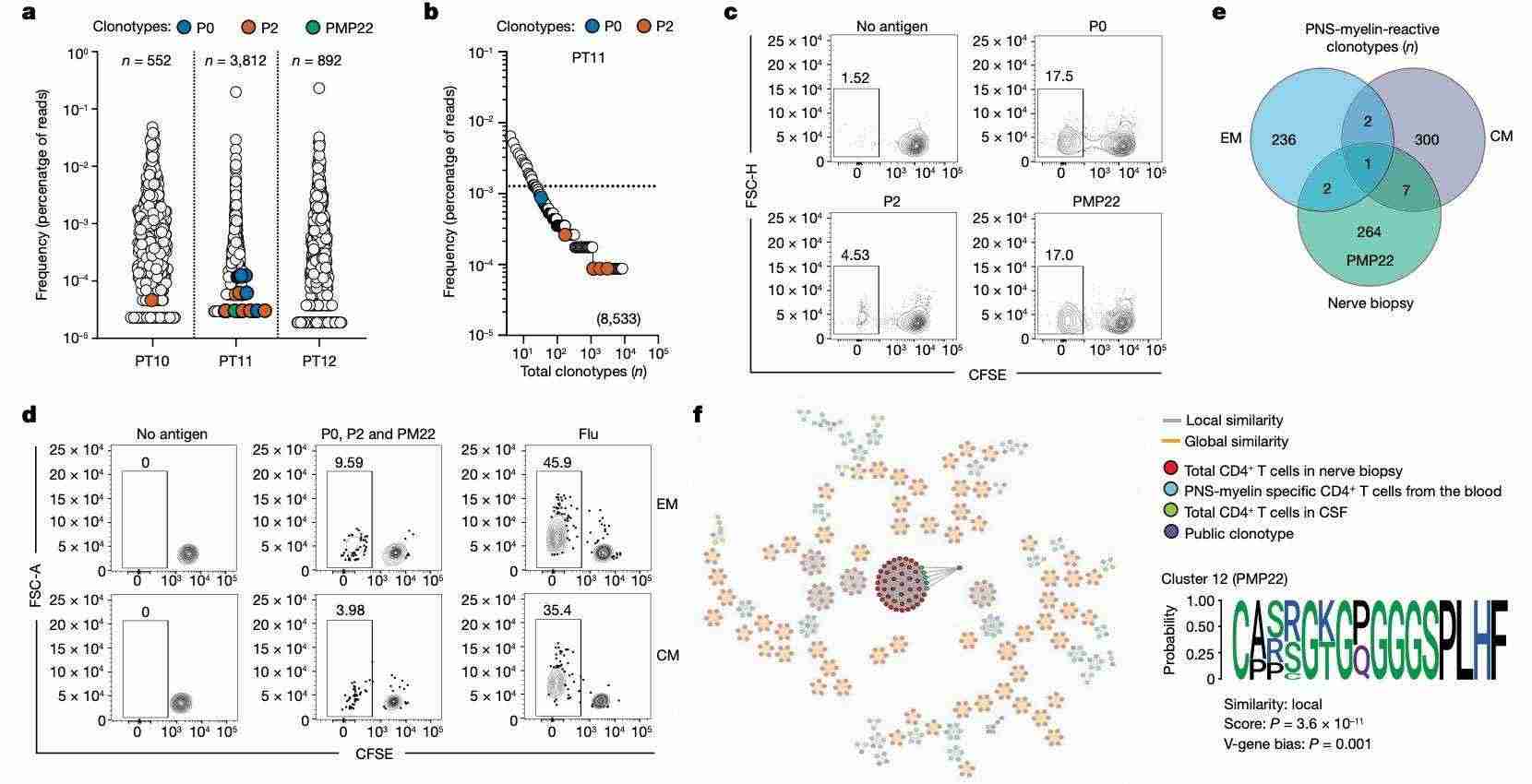
The scientists looked at how often there are special cells called 'autoreactive T cells' in the blood of patients with AIDP. They used a method called 'high-throughput TCRβ sequencing' to do this. They found these cells in some patients (PT1, PT2, PT4, PT5, PT7 and PT12). These cells were the same as special cells called 'PNS myelin-specific T cell clones'.
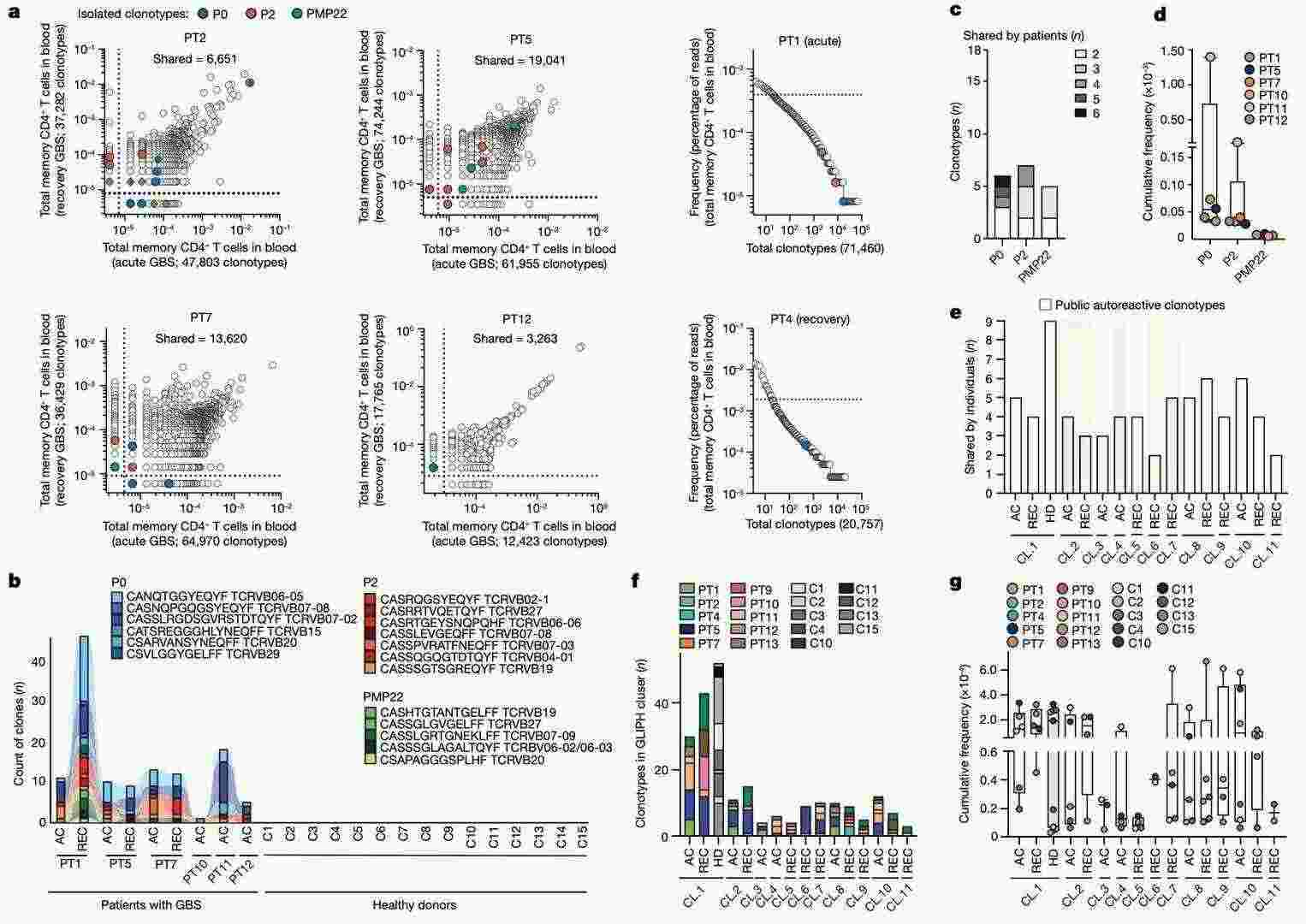 Clonotypic analysis of autoreactive T cells in patients with GBS (Súkeníková et al., 2024)
Clonotypic analysis of autoreactive T cells in patients with GBS (Súkeníková et al., 2024)
The authors also found 18 types of TCRβ cells that respond to myelin in several AIDP patients (n=6). They then looked at how these types of cells are spread out. It can be seen that the total number of shared P0-specific cells is slightly higher than that of P2- and PMP22-specific cells in patients in the early stages of the disease.
The authors then did a full analysis of TCRβ clonotypes from AIDP patients using a special algorithm (GLIPH2). This identified 11 TCRβ-specific clusters, of which only cluster 1 was shared by nine patients and nine healthy donors. However, cluster 1 did not show a higher number of specific TCRβ cells or higher frequency compared to healthy donors. These findings show that there are special cells in the blood of people with AIDP during times when the disease gets worse and better, and after recovery. These cells can be used to identify the different types of autoreactive TCRβ cells in people with AIDP.
CSF and self-reactivity in peripheral nerves
To study certain immune cells in the brain, the researchers collected fluid from the brain of three patients at the start of a certain disease. They then used a special process to look more closely at the different types of CD4+ T cells in the brain. This special process, called high-throughput TCRβ sequencing, allowed them to find certain types of CD4+ T cells in the brain that were specific to the myelin in the nervous system. Six of the 11 autoreactive cell types found in the CSF of Patient 11 were also found in their blood. However, no such cell types were found in the published TCRβ data set of CD4+ cells in the brains of narcolepsy patients.
 Identification of autoreactive CD4+ T cells in the CSF and peripheral nerves of patients with GBS (Súkeníková et al., 2024)
Identification of autoreactive CD4+ T cells in the CSF and peripheral nerves of patients with GBS (Súkeníková et al., 2024)
Finally, the researchers took a nerve sample from a patient (PT16) with early AIDP. They grew the sample in a lab and looked at the cells to see if they could find the thing that caused the problem. They found that the cells could target two proteins, P0 and PMP22. The authors also investigated the autoreactivity of two types of CD4+ T cells in the blood of this patient and showed the presence of T cells that reacted with myelin in both types.
The authors found 10 different types of T cells in nerve tissue and blood that reacted with myelin. This shows that there is a link between T cells in the blood and nerve tissue. They then used a special computer program (GLIPH2) to look more closely at the TCRβ clonotype groups of special CD4+ T cells found in the nervous system ("neural-infiltrating CD4+ T cells") from patient (PT16), special CD4+ T cells from the nervous system ("myelin-specific CD4+ T cells") from patient (PT16) blood, and all CD4+ T cells from the fluid around the brain ("total CD4+ T cells") from patients with a certain type of nerve disease called AIDP. This analysis revealed a GLIPH2 cluster and a shared PMP22-specific clonotype.
These results show that there are myelin-reactive T cells in the affected nervous tissue and fluid around the spine. This suggests that these cells may play a role in the immune problems caused by AIDP.
To sum things up, these findings give a full picture of the immune system in patients with AIDP, help us understand the causes of the immune problems in GBS, and show us how to stop the disease from getting worse and reduce the chances of death and disability.
Reference
CD Genomics is transforming biomedical potential into precision insights through seamless sequencing and advanced bioinformatics.


